



Lipedema
Consultations offered at our three convenient locations in Encino, Glendale and Bakersfield

Lipedema is an abnormal fat accumulation in lower body, usually in the buttocks, thighs, knees, and legs. Excessive fat deposition is not uniform and unproportionate. Approximately, 11% of women suffer from this disease.
Lipedema can cause pain and make daily activities difficult. Lipedema doesn’t respond to diet and exercise like ordinary fat, but there are treatments available.





Contents
Lipedema Vs. Lymphedema

Lipedema can be mistaken for obesity or lymphedema. Your body’s lymphatic system, which helps protect you against infection, moves a fluid called lymph through your body. When lymph builds up because lymph vessels or nodes that the fluid travels through are missing, damaged, or removed, that buildup is called lymphedema. Both lipedema and lymphedema can cause swelling, but lipedema is not caused by lymph buildup.
Lipedema can lead to lymphedema which is much harder to treat. With lipedema, over time, fat cells can block the vessels of your lymphatic system. This blockage prevents the proper drainage of lymph fluid, leading to lymphedema. If not treated, lymphedema can lead to problems such as infections, delayed wound healing, development of scar-like tissue called fibrosis, and hardened skin in the legs.
Unlike lymphedema, lipedema doesn’t start in the lower legs (feet and ankles) but the upper legs, and it isn’t related to prior surgery. It usually affects both legs.
Types & Stages of lipedema
You may have more than one type of lipedema at a time, depending on where you have symptoms. Types of lipedema include:
- Type I: Fat is between your belly button and your hips.
- Type II: Fat is between your pelvis and knees.
- Type III: Fat is between your pelvis and ankles.
- Type IV: Fat is between your shoulders and wrists.
- Type V: Fat is between your knees and ankles.

Lipedema Complications
The buildup of fat from lipedema can make it difficult for you to walk and move around.
Because fat from lipedema can block the lymphatic system, it can lead to lipo-lymphedema, which means you have both lipedema and lymphedema in your body.
The fat buildup with lipedema can cause joint problems, including knock knees. Lipedema may also lead to flat feet and venous (vein) disease.
Along with physical complications, lipedema can affect your quality of life, because it may contribute to depression, distress about your appearance, and feelings of embarrassment and anxiety.
Treatments of lipedema include
A. Hormone therapy in women with abnormal hormonal balance.
B. Compression stocking.
C walking and increase in activities to reduce legs swelling.
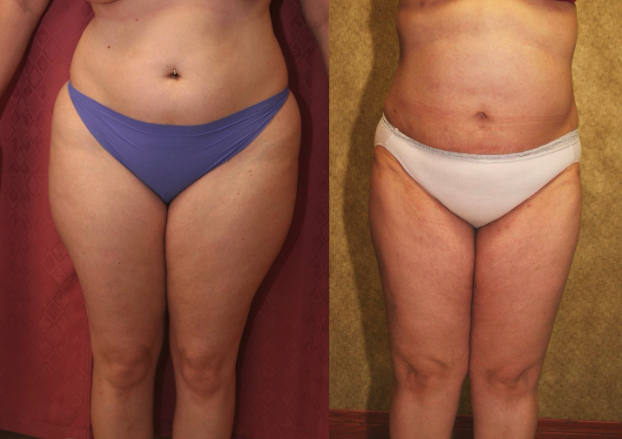
D. Large Volume Liposuction.
Large Volume Liposuction Treatment of Lipedema
Dr. Younai is a Board-certified Plastic Surgeon for over 25 years’ experience in the treatment of Lipedema using large volume liposuction. Dr. Younai’s goal has been to enable patients to get a more proportionate figure and become more functional so that they can live better lives.